Enteral nutrition (EN) is provided for patients that have a functioning lower gastrointestinal (GI) tract but are unable to orally ingest nutrients and medication and are at risk for malnutrition.[1] Feeding tubes (Tubes) provide these patients essential nutrition, life-sustaining medications and hydration. Numerous conditions may necessitate long-term EN, including GI dysfunction, cancer, cystic fibrosis, neurological disorders, burn patients, congenital heart disease, Alzheimer’s disease, Parkinson’s disease, and congenital metabolic abnormalities.[1,2] Maintaining Tube patency is critical for many, as EN interruptions are often associated with poor clinical outcomes. Tube clogging (see Figure 1) is the most frequently reported mechanical complication associated with feeding tubes, with reported clogging rates ranging from 9-35%.[3-5] A recent survey of Oley Foundation members (180+ patients with feeding tubes and/or caretakers) indicated that up to 81% of non-acute Tubes become clogged, with 39.4% requiring a tube replacement due to clogs.[6] Clogs result in the interruption of patient’s nutrition and medication regimens, representing a burden to both caregivers and patients.
Figure 1: Images of actual clogged feeding tubes submitted by three (3) different hospitals to Actuated Medical, Inc.
Common approaches to maintain Tube patency include regular flushing with water, carbonated sodas, and enzymatic solutions immediately after administering nutrition or medication. Some healthcare facilities add procedures for adequately crushing medications to prevent clogs. Current methods for unclogging Tubes are time-consuming and unreliable, often ending in patients having to undergo Tube replacements. Tube replacements are associated with their own set of risks, including the need for patient transport to the hospital, transfer to interventional radiology (IR) for radiological guidance or Tube placement confirmation following placement, exposing patients to radiation exposure, or surgical interventions which can expose patients to anesthesia.[7-10] Moreover, Tube misplacements into the bronchial tree reportedly occur in 2.4-3.2% of all nasogastric (NG) tube insertions,[11] a serious complication which, if unidentified, results in pneumonitis, pneumonia, and/or pneumothorax.[11]
Actuated Medical, Inc. (AMI) aimed to directly compare the prophylactic use of the TubeClear system, an actuated mechanical clearing device, to standard practice water flushes at reducing inner wall Tube material buildup, as a means of reducing subsequent material adherence and Tube clogging in vitro. Establishing protocols that could minimize clog formation would be invaluable for maintaining Tube patency and allowing for nutrition and medication regimens to remain uninterrupted.
Methods
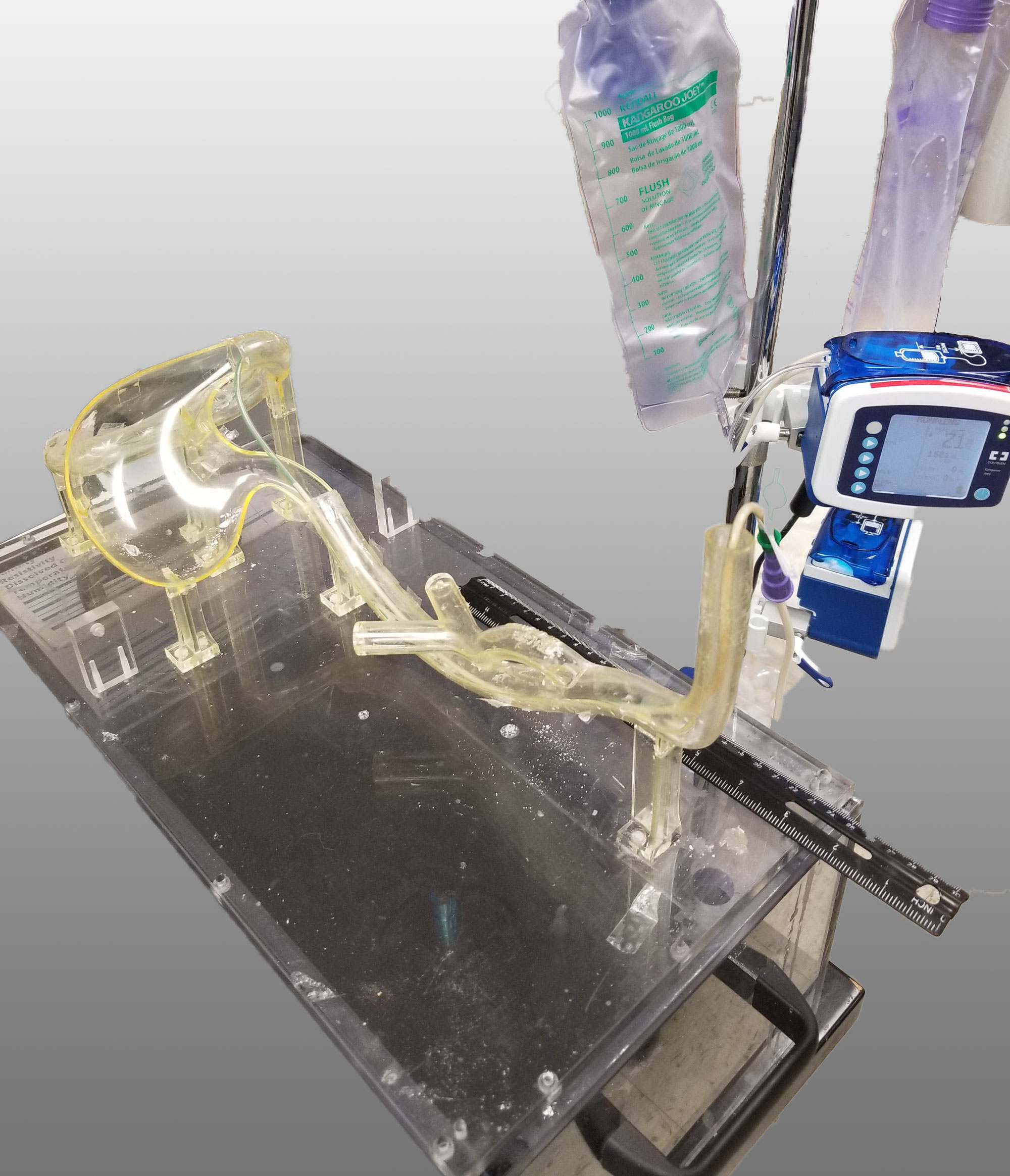
Nasogastric (NG) tubes (N=22, 10Fr, 42”) were partially clogged with feeding formula and fiber supplement mixture. Mixture was introduced and blown through with air, coating the Tube inner walls and dried (55°C for 3 hrs.). Tubes were placed in a 3D gastrointestinal model and pump fed (21 mL/hr.) until Tube length was entirely filled with formula (see Figure 2). Half of the Tubes (n=11) were subsequently flushed with 30 mL of water, as directed by clinical practice following feeding formula introduction. The other half of tubes (n=11) underwent a 30 mL water flush in coordination with use of the TubeClear system according to the manufacturer’s instructions. Following clearing procedures, Tubes were dried (55°C for 3 hrs.) to remove moisture introduced by water flushes. Tubes were weighed before and after mixture introduction to quantify the mass within Tubes. As such, the final recorded masses within Tubes were a combination of the initial introduced mixture and added pump fed formula. These mean values did not differ by clearing treatment (0.248 vs 0.250 g, Water vs TubeClear, unpaired T-test, p=0.76) prior to drying. Tubes were weighed following clearing and drying and percent mass increase or decrease from initial mixture mass were calculated (see Figure 3).
Figure 2: Tube in GI model being pumped with formula.
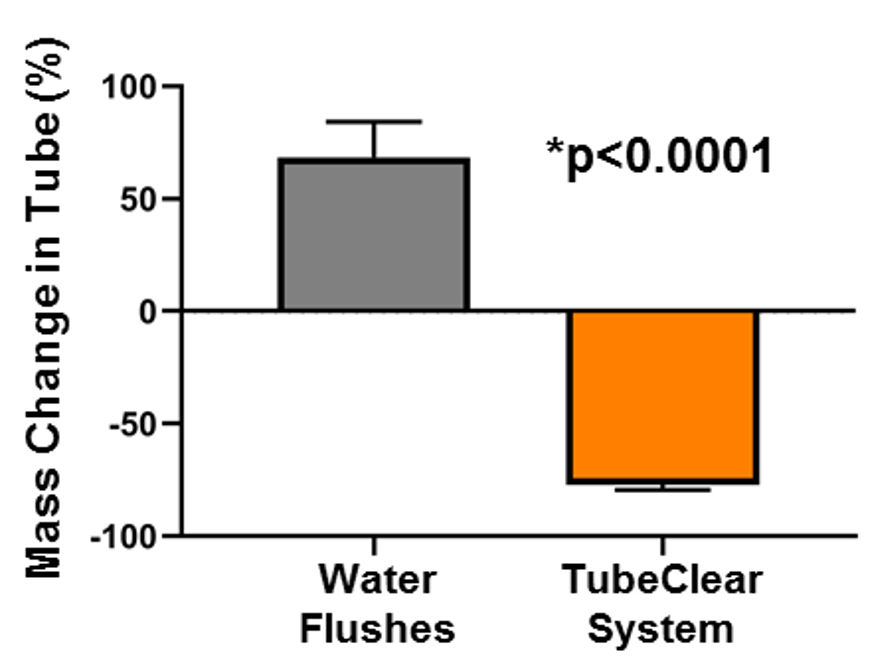
Figure 3: Percent change in mass of NG tubes flushed with with either water alone (Gray Bar) or in conjunction of the TubeClear system (Orange Bar) to remove buildup residue within Tube inner walls. N=22, 11/treatment; Unpaired T-test for significance, Bars= standard error of the mean. *p <0.0001.
Results
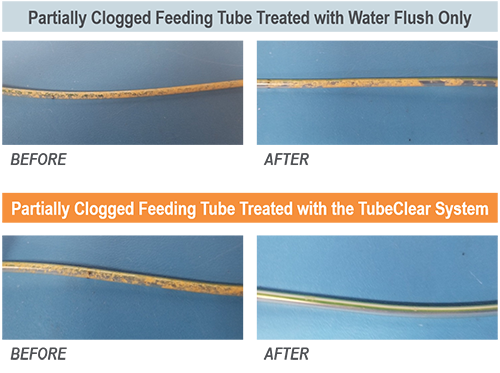
The TubeClear system in conjunction with water flushes removed 77.1±2.4% of mass while Water flushing alone added 68.5±15.8% (see Figure 3, unpaired T-test p<0.0001).[12] As added water was removed by post-clearing drying, the added mass, in Water group, was likely formula sticking to the pre-existing Tube material buildup. Images of the partially clogged feeding tubes treated with water or combined with the TubeClear system demonstrated visual differences (see Figure 4), confirmed with mass measurements.
All Tubes cleared by TubeClear decreased in mass, while nearly all the Tubes flushed with water alone, increased in mass.
The TubeClear system was 145.6% more effective than water alone at removing buildup.
Figure 4: Representative examples of partially clogged feeding tubes treated with water alone (top) or in conjunction with the TubeClear system (Bottom) to remove buildup residue within Tube inner walls.
Conclusions
This work demonstrates that compared to water flushes alone, proactive use of the TubeClear system prior to Tube occlusions can minimize added material buildup from adhering to Tube inner walls, maintaining full Tube diameter and reducing the risk of future clogging, enabling uninterrupted and optimal EN delivery.
References:
Ireton-Jones C, DeLegge M. Handbook of Home Nutrition Support. Sudburry, MA: Jones and Bartlett; 2007.
Shiram K, Jayanth, V., Lakshmi, R., George, V. Prophylactic Locking of Enteral Feeding Tubes With Pancreatic Enzymes. Journal of Parenteral and Enteral Nutrition. 2012;21(6):353-356.
Oley Foundation Member Survey: Enteral Feeding Tube Clogging and Resolution. In: Actuated Medical, Inc.; 2015.
Mathus-Vliegen L, Koning H. Percutaneous endoscopic gastrostomy and gastrojejunostomy: a critical reappraisal of patient selection, tube function and the feasibility of nutritional support during extended follow-up. Gastrointest Endosc. 1999;50(6):746-754.
Sy K, Dipchand A, Atenafu E, et al. Safety and effectiveness of radiologic percutaneous gastrostomy and gastro jejunostomy in children with cardiac disease. AJR Am J Roentgenol. 2008;191(4):1169-1174.
Towbin R, Ball WJ, Bissett Gr. Percutaneous gastrostomy and percutaneous gastrojejunostomy in children: antegrade approach. Radiology. 1988;168(2):473-476.
Many people think feeding tubes are merely used to deliver nutrition (i.e., feeding formula), however, they deliver life-sustaining medications too – it’s no wonder they tend to clog. At Actuated Medical, Inc., we developed the TubeClear System to keep enteral therapy (medication, nutrition and hydration) being delivered as prescribed.
i
Article Summary
Forces required to do air flushes via enteral syringe in feeding tubes with no clog, 1-layer, and 2-layers of feeding formula mixtures were measured.
Feeding tube clogs, or material build-up on the walls (i.e., 1-layer clogs), may begin forming before becoming noticeably difficult to flush.
2-layer clogs required a force that was nearly 5.5 times of the “No Clog” feeding tubes, which was noticeable when flushed by hand.
The TubeClear System should be used when caregivers notice higher forces during air or water flushes to maintain full patency of feeding tubes.
We have demonstrated that compared to flushing with water alone, the TubeClear System can remove residue “sludge” from feeding tube interior walls with greater efficacy.[1] However, the question remains – How does one know when material build-up is adhering to the interior feeding tube wall if fluids can still be introduced into the feeding tube?
For patients using feeding pumps, most pump alarms will sound an alert when the flow rate falls below the predesignated flow rate.[2] However, for those using gravity or syringe feedings, clinicians flush the feeding tube with a syringe to confirm patency (open or unobstructed). These water flushes may require increased force if materials are building up on the inner tube walls. In cases of fully clogged feeding tubes, the water may blow backward toward the clinician due to increased syringe resistance. Note that using excessive force on a syringe (often called power flushing) is generally not recommended as it may cause a rupture to the patient’s feeding tube.[3]
Measuring Flushing Force
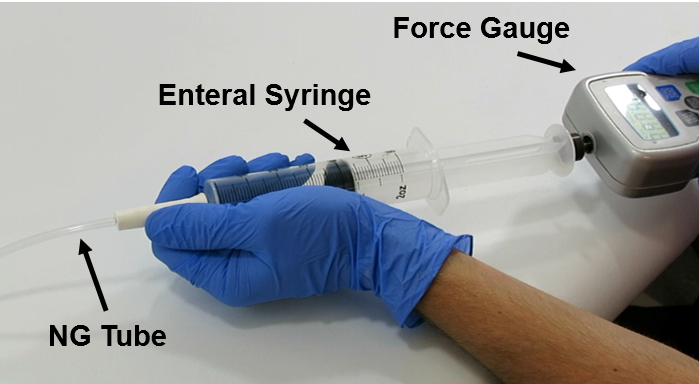
Our engineers investigated the amount of force (Newtons [N]) required to be applied to a syringe plunger when attempting to introduce air into non-clogged and partially clogged feeding tubes. In vitro produced clogs were created with a mixture of feeding formula and fiber within 14Fr NG feeding tubes (Cardinal Health, Dublin, OH). Three (3) different feeding tube conditions were tested, N=15 trials, with n=5 trials/feeding tube condition: 1) No clog (lacking all material), 2) 1-layer of clog mixture on feeding tube walls, and 3) 2-layers of clog mixture on feeding tube walls (see Figure 2). To create the single layer, the clog mixture was introduced into feeding tubes (N=10) and dried at 55°C for three (3) hours. To create the two-layer clog buildup, a second clog layer was introduced into a subset of the same feeding tubes (N=5) and dried at 55°C for three (3) hours. To measure the force, a 60-cc syringe was filled with air to the 50-cc mark, and the plunger was depressed to the 10-cc mark using a Shimpo model 100XY force gauge (ELECTROMATIC Equipment Co., Inc., Cedarhurst, NY) (see Figure 1). A n = 5 trials were performed for each feeding tube condition.
Figure 1: Testing set-up.
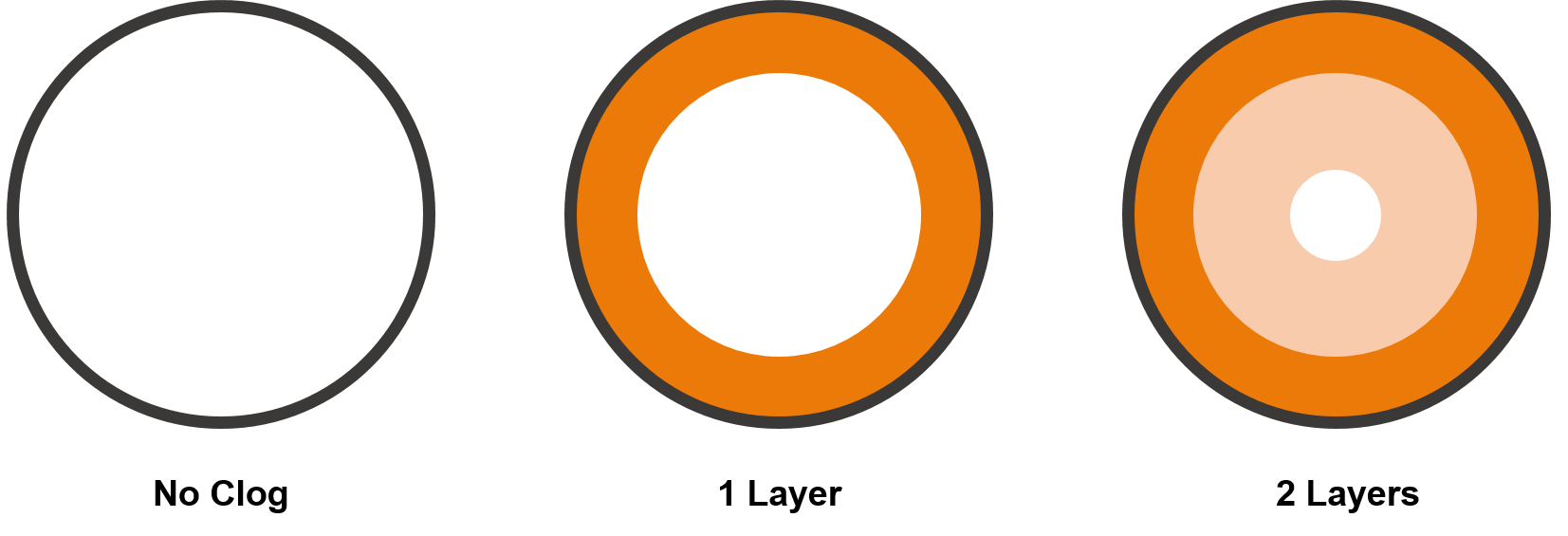
Figure 2: A rendering of the cross-section of the clog types. The grey circle represents the feeding tube wall, and clog material is represented in shades of orange.
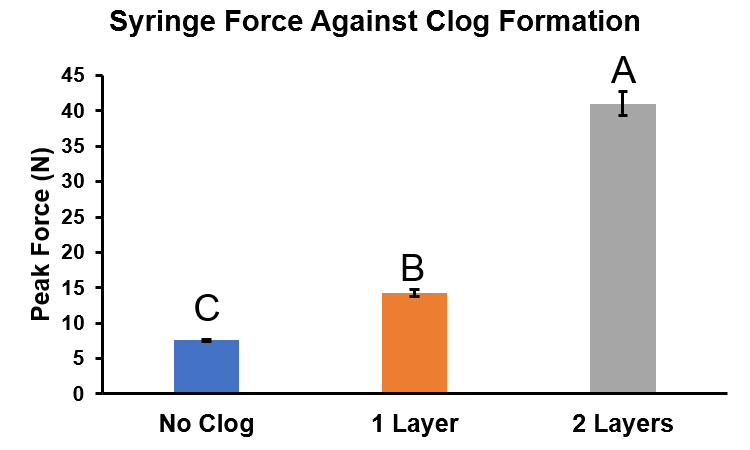
The peak force (measured in Newtons [N]) required to push air via the syringe through a non-clogged feeding tube averaged 7.6±0.1N, compared to 14.3±0.5N and 41.0±1.7N, for the one and two layered partially clogged feeding tubes, respectively (see Figure 3).
While these measurements demonstrate an increasing amount of required force, what does that feel like in practice?
Figure 3: Syringe Force testing summary. Blue Bar= No clog, Orange Bar= Single layer of clog mixture, Gray Bar= Double layer of clog mixture. n=5 trials/performed for each feeding tube condition. Error bars= standard error of the mean. Two-way ANOVA, Tukey’s Multiple comparison test, different variables =p<0.01.
Feeling the Force
There are many publications discussing preventative means to feeding tube clog formation and multiple ways to remove clogs;[4-5] however, the question as to how one can determine if a feeding tube is fully patent does not appear to have been addressed.
Some feeding tube clogs appear to form quickly, while others occur gradually over time, leading clinicians and care takers to be uncertain to the state of patency of a feeding tube at any particular time. We aimed to quantify the amount of required force to introduce air into feeding tubes with the various levels of clogging- with the end goal to correlate those values with a subjective “feel,” as such, initial tests were conducted without a force gauge. Videos demonstrate how easily (or not) air could be introduced into feeding tubes of the various conditions.
A
B
C
Figure 4: Syringe resistance against each feeding tube condition. A) No clog. B) 1 layer. C) 2 layers (note: looping GIF animation may look like the plunger “snaps” back, but this is the beginning of the animation).
As expected, the feeding tube without a clog (No Clog) could be flushed with air without experiencing any major resistance. However, the feeding tube with a single layer of clog mixture appears to flush almost as easily as the “No Clog” feeding tube, but the required force as measured by the force gauge was nearly double. This finding suggests that feeding tube clogs, or material build-up on the walls, may begin forming before becoming noticeable to clinicians or caretakers. Further research is required to elucidate this finding.
Attempts to flush air into feeding tubes with a double layer of clog mixture proved the most difficult, requiring additional force as the syringe plunger pushed backwards towards the Operator (see Figure 4c) due to the partial blockage. These simulated clogs required a force that was nearly 5.5 times that of the “No Clog” feeding tubes.
From Bench to Bedside
Using the TubeClear System proactively can remove material build-up from feeding tube inner walls enabling enteral therapy (i.e., medication, nutrition and hydration) to be delivered as prescribed.[1] Based on the results presented here, we recommend using the TubeClear System on a patient’s feeding tube as soon as the clinician notices a change in the required pressure to administer fluid or air during routine syringe flushing, as this may be indicative of material build-up on the inner walls of the tube.
References:
Actuated Medical, Inc. Internal Test Report Doc. No. 1100791569-001.
Boullata, J. I., Carrera, A. L., Harvey, L. , Escuro, A. A., Hudson, L. , Mays, A. , McGinnis, C. , Wessel, J. J., Bajpai, S. , Beebe, M. L., Kinn, T. J., Klang, M. G., Lord, L. , Martin, K. , Pompeii‐Wolfe, C. , Sullivan, J. , Wood, A. , Malone, A. , Guenter, P. and , (2017), ASPEN Safe Practices for Enteral Nutrition Therapy. Journal of Parenteral and Enteral Nutrition, 41: 15-103 0148607116673053. doi:1177/0148607116673053.
Lord, L.M. (2018), Enteral Access Devices: Types, Function, Care, and Challenges. Nutrition in Clinical Practice, 33(1): 16-38. doi: 10.1002/ncp.10019.
Enteral access devices (EADs; feeding tubes) provide vital nutrition, medication, and hydration to more than seven million patients annually [1]. Interruptions to the delivery of enteral therapy has been found to increase the patient’s caloric deficit and their hospital length of stay[2], greatly increasing the overall cost of care.
The TubeClear System, a device developed to clear clogged or
sluggish feeding tubes to restore or maintain their patency, could help prevent
interruptions to delivery of enteral therapy when used proactively. A recent bench test found promising results.[3]
Bench studies suggest that, when used correctly and
proactively (i.e. before a feeding tube becomes completed clogged), the
TubeClear System is 145.6% more effective at removing built-up material along
the walls of the feeding tube than the standard practice of flushing a tube
with water. As material builds up along the inside walls of the feeding tube,
it can gradually restrict the flow of nutrition.
Actuated Medical, Inc. (AMI) tested the use of the TubeClear System on partially clogged feeding tubes. For this test, 22 feeding tubes were used; the patency of 11 tubes was maintained with the standard practice of water flushing, and the patency of the other 11 tubes was maintained with the TubeClear system. A weight was recorded for each empty feeding tube before it was clogged. The clog contents included a combination of feeding formula and fiber supplements, to simulate types of clogs observed in a clinical setting, and clogged feeding tubes were then dried to ensure consistency between the tubes. Each clogged tube was weighed and received a water flush.
For the first 11 feeding tubes, only water was used for
clearing the tube. After treatment, they
were weighed again. On average, flushing
the partial clog with water increased
the weight of the feeding tube by 68.5%, indicating that the moisture may
have been absorbed by the build-up.
The second 11 feeding tubes were treated with the TubeClear System
after the initial water flush. On
average, those feeding tubes decreased
in weight by 77.1%, suggesting more of the occlusion material was removed
than the tubes treated with water alone.
These results suggest that the TubeClear System is more
effective at clearing partial clogs than the standard practice of flushing with
water alone. AMI recommends using the
TubeClear System at least once per week for optimum therapy delivery. If the flow within the feeding tube is
sluggish in the meantime, indicated by a feeding pump alarm or when it’s
difficult to flush with water or administer medication, it is appropriate to
use the TubeClear System more frequently, as needed.
[1]
Botoman VA, Kirtland SH, Moss RL. “A randomized study of a pH sensor feeding
tube vs a standard feeding tube in patients requiring enteral nutrition”, JPEN
J Parenter Enteral Nutr. 1994;18(2):154-158.
[2]
Peev, M. P., Yeh, D. D., Quraishi, S. A., Osler, P. , Chang, Y. , Gillis, E. ,
Albano, C. E., Darak, S. and Velmahos, G. C. (2015), Causes and Consequences of
Interrupted Enteral Nutrition. Journal of Parenteral and Enteral Nutrition, 39:
21-27. doi:10.1177/0148607114526887
[3]
Source: Actuated Medical, Inc. Internal Test Report Doc. No. 1100791569-000.
Small bore feeding tubes are used to provide essential nutrition and medication to patients at risk of malnutrition and dehydration due to an inability to ingest orally (1).
Clogging is one of the most frequent mechanical complications of feeding tubes (2,3). Tubes are more likely to become clogged when powdered, crushed, acidic, or alkaline medications or ground feeding formulas containing particulates are delivered through the small inner lumen, or when tubes are not routinely flushed following feedings (2). Reported clogging rates vary, ranging from 9-35% (1, 2).
Attempts to clear clogged feeding tubes using various techniques are time-consuming and often result with tube replacement still being required. Also, many of the current methods only work on certain types of clogs. For example, most enzyme treatments are only applicable to protein (feeding formula) based clogs. Among common emergency room medical procedures, patients rank nasoenteral (NE), (nasogastric [NG]) tube insertion to be one of the most painful (4, 5, 6). Replacing a feeding tube may cause additional patient safety risks, associated medical costs, and additional pain and discomfort to the patient. The most common way to place NE (NG) feeding tubes, is blind insertion at patient bedside, and has a reported 0.5-15% malposition rate (3). Malposition into the trachea may cause pneumothoraxes and possibly death. Several methods exist for verifying accurate tube placement, the most reliable being radiography (3). However, this exposes patients to additional radiation and medical costs.
Taking into account nursing time, tube replacement, radiographs and other miscellaneous costs, the capability to clear a clogged feeding tube while it remains in the patient, could represent substantial savings to a medical facility not to mention reduced pain and discomfort to the patient. For patients outside the hospital, a clogged feeding tube often results in transportation and admission costs to the payer and anxiety to the patient.
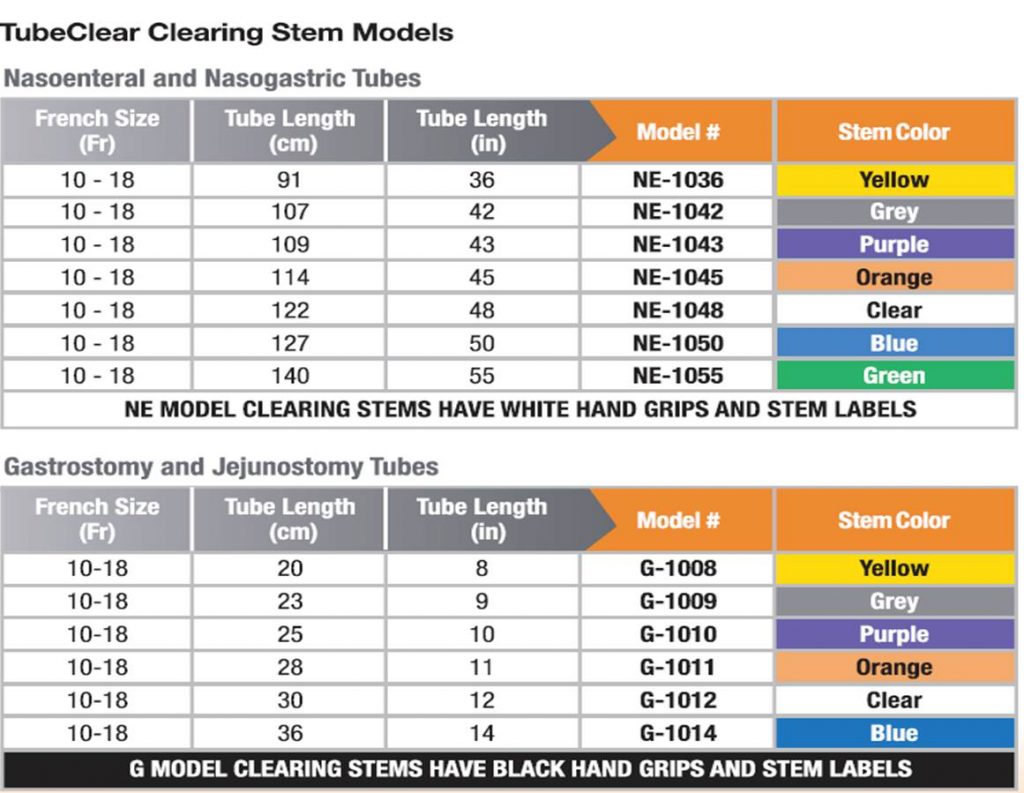
The TubeClear System was developed to efficiently and effectively clear clogged feeding tubes while the tube remains in the patient (7). It is currently FDA cleared to unclog 10-18 Fr NE, NG, gastrostomy (G [including percutaneous endoscopic gastrostomy, PEG tubes]) and jejunostomy (J) feeding tubes in adults at bedside while the tube remains in the patient. The TubeClear System is also CE marked. The TubeClear System is comprised of a reusable Control Box to which a single-use Clearing Stem is attached. The Clearing Stem is inserted into the patient’s feeding tube by the licensed healthcare practitioner. The Clearing Stem moves backward and forward, and the tip works against the clog to mechanically disrupt and clear the feeding tube.
+ FDA Cleared for clearing occlusions / clogs in Feeding and Decompression Tubes in adult patients that have a Tube size of 6 to 18 Fr.
References:
1. Ireton-Jones C, DeLegge M. Handbook of Home Nutrition Support. Sudburry, MA: Jones and Bartlett; 2007
2. Beyer PL, Matarese LE, Gottschlich MM. Complications of enteral nutrition. 1998.
3. Blumenstein I, Shastri YM, Stein J. Gastroenteric tube feeding: techniques, problems and solutions. World J Gastroenterol. 2014;20(26):8505-8524.
4. Singer AJ, Richman PB, Kowalska A, Thode HC, Jr. Comparison of patient and practitioner assessments of pain from commonly performed emergency department procedures. Ann Emerg Med. 1999;33(6):652-658.
5. Bae KH, Jeong IS. [Pain perception of nurses and pain expression of patients in critical care units]. J Korean Acad Nurs. 2014;44(4):437-445.
6. Penrod J, Morse JM, Wilson S. Comforting strategies used during nasogastric tube insertion. J Clin Nurs. 1999;8(1):31-38.
7. TubeClear System- Clears Clogged Feeding Tubes. 2015;https://www.tubeclear.com/
Individuals unable to ingest nutrition and/or medication orally for various causes, often become dependent on enteral nutrition as a life-saving mechanism (1). However, due to daily administration of feeding formula and/or medication, as well as other unknown causes, these medically needed feeding tubes may become clogged, up to 35% of the time (1, 2).
Clogged feeding tubes often result in the interruption of a patient’s nutrition and medication regimens, representing a burden to both caregivers and patients. Attempts to clear clogged feeding tubes using various techniques are time-consuming and as a result cause delays in feeding, hydration, and medications which can have negative effects on overall patient health and healing (3). Often, these tube clearing methods fail and the tube requires replacement, exposing patients to both additional radiation from placement confirmation (x-rays) and increased medical costs. Notably, among common medical procedures, patients rank nasoenteral (NE), (nasogastric [NG]) tube insertion to be one of the most painful (4, 5, 6). The most common way to place NE (NG) feeding tubes, is blind insertion, and has a reported 0.5-16% malposition rate (7). Malposition into the trachea may cause pneumothoraxes and possibly death, though several methods exist for verifying accurate placement, the most reliable is radiography (7). Replacing clogged gastrostomy (G) and jejunostomy (J) feeding tubes may require additional endoscopic guidance or surgical procedures depending on tube type.
The TubeClear System, an FDA-cleared and CE marked medical device, was developed to clear clogged feeding tubes at bedside while the tube remains in the patient. The system comprises of a reusable Control Box that actuates a single-use Clearing Stem. The Clearing Stem inserts into the feeding tube and the backward and forward movement of the Clearing Stem acts to mechanically disrupt and clear the clogged feeding tube (8). It is currently FDA cleared to unclog 6-18 Fr NE, NG, G (including percutaneous endoscopic gastrostomy, [PEG tubes]) and J tubes while the tube remains in the patient.
+ FDA Cleared for clearing occlusions / clogs in Feeding and Decompression Tubes in adult patients that have a Tube size of 6 to 18 Fr.
Using the TubeClear System to Clear Clogged G-tubes.
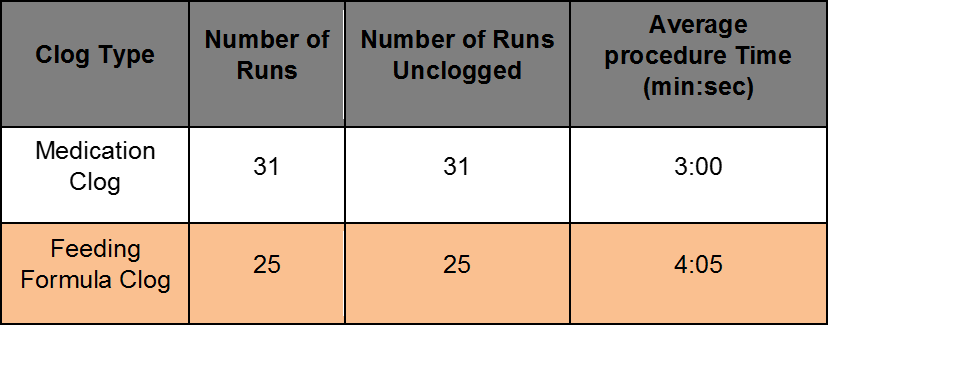
Benchtop Study evaluated at AMI with Levin 18 Fr, 14 inch long gastrostomy tubes. Half of the occlusions were made from 2:1 ratio of coagulated protein and ground medication (Medication Clog). Half of the occlusions were made from 1:1 ratio of feeding formula and fiber (Feeding Formula Clog).
Using the TubeClear System to Clear Clogged NE tubes.
Benchtop Study evaluated at AMI with Levin 10F Fr, 55 inch long nasoenteral (Entriflex) tubes. Half of the occlusions were made from 2:1 ratio of coagulated protein and ground medication (Medication Clog). Half of the occlusions were made from 1:1 ratio of feeding formula and fiber (Feeding Formula Clog).
References:
1. Ireton-Jones C, DeLegge M. Handbook of Home Nutrition Support. Sudburry, MA: Jones and Bartlett; 2007
2. Beyer PL, Matarese LE, Gottschlich MM. Complications of enteral nutrition. 1998.
3. Pearce C, Duncan H. Enteral feeding. Nasogastric, nasojejunal, percutaneous endoscopic gastrostomy, or jejunostomy: its indications and limitations. Postgrad Med J. 2002;78(918):198-204.
4. Singer AJ, Richman PB, Kowalska A, Thode HC, Jr. Comparison of patient and practitioner assessments of pain from commonly performed emergency department procedures. Ann Emerg Med. 1999;33(6):652-658.
5. Bae KH, Jeong IS. [Pain perception of nurses and pain expression of patients in critical care units]. J Korean Acad Nurs. 2014;44(4):437-445.
6. Penrod J, Morse JM, Wilson S. Comforting strategies used during nasogastric tube insertion. J Clin Nurs. 1999;8(1):31-38.
7. Blumenstein I, Shastri YM, Stein J. Gastroenteric tube feeding: techniques, problems and solutions. World J Gastroenterol. 2014;20(26):8505-8524.
8. TubeClear System- Clears Clogged Feeding Tubes. 2015;https://www.tubeclear.com/
Small bore feeding tubes are used to provide essential nutrition and medication to patients at risk of malnutrition and dehydration due to an inability to ingest orally (1). Clogging is one of the most frequent mechanical complications of feeding tubes (2,3). Tubes are more likely to become clogged when powdered, crushed, acidic, or alkaline medications or ground feeding formulas containing particulates are delivered through the small inner lumen, or when tubes are not routinely flushed following feedings (2).
Clearing clogged feeding tubes creates hassles and frustration for practitioners and anxiety and discomfort for patients. The lapse in nutrition and medication regime may also negatively impact recovery (4). Standard techniques for clearing clogged feeding tubes in the past included enzymes, Coca-Cola®, and meat tenderizer. Today, commercially available manual brushes and stylets exist, in addition to enzymes or syringe water flushes (2,5,6). Attempts to clear clogged feeding tubes using these techniques are time-consuming and often result with tube replacement still required. Moreover, among other common medical procedures, patients rank Nasoenteral (NE, nasogastric [NG]) tube insertion to be one of the most painful (7,8,9).
The TubeClear System, an FDA-cleared and CE marked medical device, was developed to clear clogged feeding tubes at bedside while the tube remains in the patient. The system comprises of a reusable Control Box that actuates a single-use Clearing Stem. The Clearing Stem inserts into the feeding tube and the backward and forward movement of the Clearing Stem acts to mechanically disrupt the clog and clear the clogged feeding tube (10).
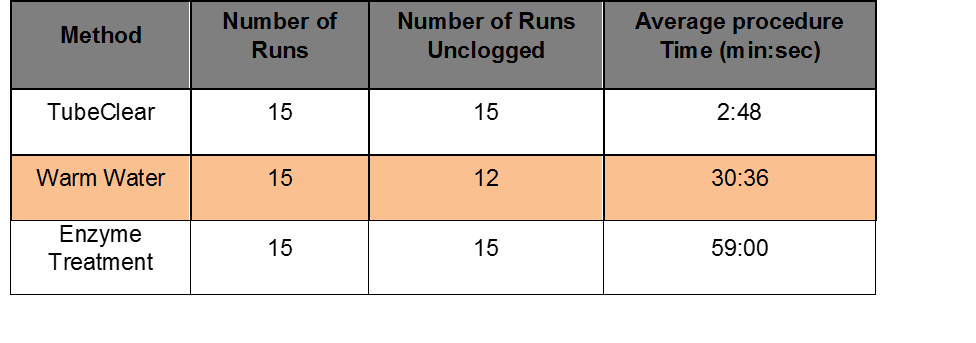
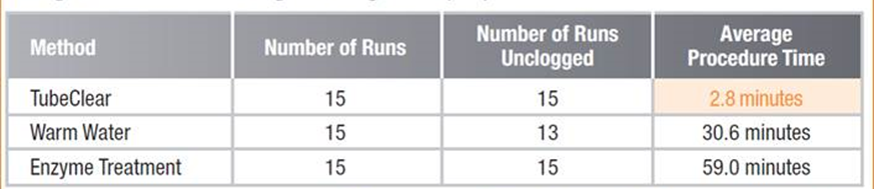
A bench study was conducted to test the efficacy of three different clog-clearing strategies on in-vitro clogged tubes. Of the three clog clearing strategies tested with artificially clogged tubes, warm water flushes and commercially available enzyme treatments took significantly longer to clear clogged feeding tubes, when compared to the TubeClear System.
FDA Cleared for clearing occlusions / clogs in Feeding and Decompression Tubes in adult patients that have a Tube size of 6 to 18 Fr.
Using TubeClear to Unclog Nasoenteral tubes that reside in the stomach.
Benchtop Study evaluated at AMI with Levin 14Fr, 48 inch long feeding tubes with in-vitro clogs. Occlusions were made from 1:1 ratio of feeding formula and fiber.
References:
Ireton-Jones C, DeLegge M. Handbook of Home Nutrition Support. Sudburry, MA: Jones and Bartlett; 2007
Beyer PL, Matarese LE, Gottschlich MM. Complications of enteral nutrition. 1998.
Blumenstein I, Shastri YM, Stein J. Gastroenteric tube feeding: techniques, problems and solutions. World J Gastroenterol. 2014;20(26):8505-8524.
Pearce C, Duncan H. Enteral feeding. Nasogastric, nasojejunal, percutaneous endoscopic gastrostomy, or jejunostomy: its indications and limitations. Postgrad Med J. 2002;78(918):198-204.
Metheny N, Eisenberg P, McSweeney M. Effect of feeding tube properties and three irrigants on clogging rates. Nurs Res. 1988;37(3):165-169.
Smith R, Myers S. 2 devices that unclog feeding tubes. RN. 2005;68(1):36-41; quiz 42.
Singer AJ, Richman PB, Kowalska A, Thode HC, Jr. Comparison of patient and practitioner assessments of pain from commonly performed emergency department procedures. Ann Emerg Med. 1999;33(6):652-658.
Bae KH, Jeong IS. [Pain perception of nurses and pain expression of patients in critical care units]. J Korean Acad Nurs. 2014;44(4):437-445.
Penrod J, Morse JM, Wilson S. Comforting strategies used during nasogastric tube insertion. J Clin Nurs. 1999;8(1):31-38.



 Attempts to clear clogged feeding tubes using various techniques are time-consuming and often result with tube replacement still being required. Also, many of the current methods only work on certain types of clogs. For example, most enzyme treatments are only applicable to protein (feeding formula) based clogs. Among common emergency room medical procedures, patients rank nasoenteral (NE), (nasogastric [NG]) tube insertion to be one of the most painful (4, 5, 6). Replacing a feeding tube may cause additional patient safety risks, associated medical costs, and additional pain and discomfort to the patient. The most common way to place NE (NG) feeding tubes, is blind insertion at patient bedside, and has a reported 0.5-15% malposition rate (3). Malposition into the trachea may cause pneumothoraxes and possibly death. Several methods exist for verifying accurate tube placement, the most reliable being radiography (3). However, this exposes patients to additional radiation and medical costs.
Attempts to clear clogged feeding tubes using various techniques are time-consuming and often result with tube replacement still being required. Also, many of the current methods only work on certain types of clogs. For example, most enzyme treatments are only applicable to protein (feeding formula) based clogs. Among common emergency room medical procedures, patients rank nasoenteral (NE), (nasogastric [NG]) tube insertion to be one of the most painful (4, 5, 6). Replacing a feeding tube may cause additional patient safety risks, associated medical costs, and additional pain and discomfort to the patient. The most common way to place NE (NG) feeding tubes, is blind insertion at patient bedside, and has a reported 0.5-15% malposition rate (3). Malposition into the trachea may cause pneumothoraxes and possibly death. Several methods exist for verifying accurate tube placement, the most reliable being radiography (3). However, this exposes patients to additional radiation and medical costs.