Individuals unable to ingest nutrition and/or medication orally for various causes, often become dependent on enteral nutrition as a life-saving mechanism (1). However, due to daily administration of feeding formula and/or medication, as well as other unknown causes, these medically needed feeding tubes may become clogged, up to 35% of the time (1, 2).
Clogged feeding tubes often result in the interruption of a patient’s nutrition and medication regimens, representing a burden to both caregivers and patients. Attempts to clear clogged feeding tubes using various techniques are time-consuming and as a result cause delays in feeding, hydration, and medications which can have negative effects on overall patient health and healing (3). Often, these tube clearing methods fail and the tube requires replacement, exposing patients to both additional radiation from placement confirmation (x-rays) and increased medical costs. Notably, among common medical procedures, patients rank nasoenteral (NE), (nasogastric [NG]) tube insertion to be one of the most painful (4, 5, 6). The most common way to place NE (NG) feeding tubes, is blind insertion, and has a reported 0.5-16% malposition rate (7). Malposition into the trachea may cause pneumothoraxes and possibly death, though several methods exist for verifying accurate placement, the most reliable is radiography (7). Replacing clogged gastrostomy (G) and jejunostomy (J) feeding tubes may require additional endoscopic guidance or surgical procedures depending on tube type.
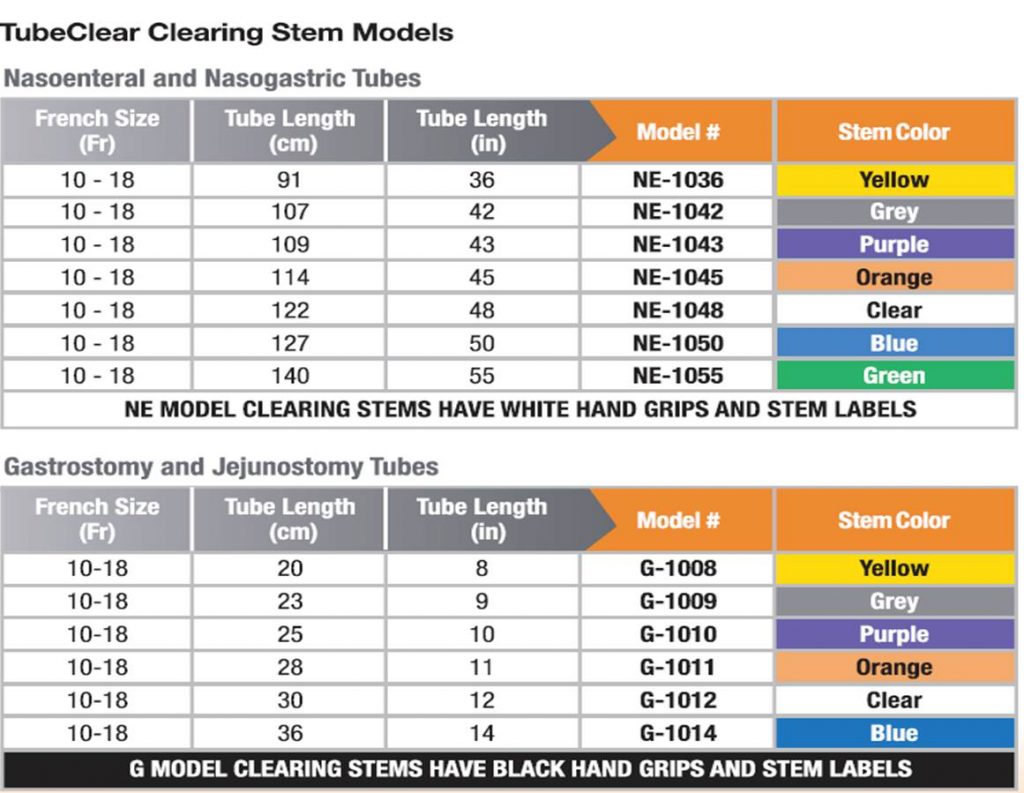
The TubeClear System, an FDA-cleared and CE marked medical device, was developed to clear clogged feeding tubes at bedside while the tube remains in the patient. The system comprises of a reusable Control Box that actuates a single-use Clearing Stem. The Clearing Stem inserts into the feeding tube and the backward and forward movement of the Clearing Stem acts to mechanically disrupt and clear the clogged feeding tube (8). It is currently FDA cleared to unclog 6-18 Fr NE, NG, G (including percutaneous endoscopic gastrostomy, [PEG tubes]) and J tubes while the tube remains in the patient.
+ FDA Cleared for clearing occlusions / clogs in Feeding and Decompression Tubes in adult patients that have a Tube size of 6 to 18 Fr.
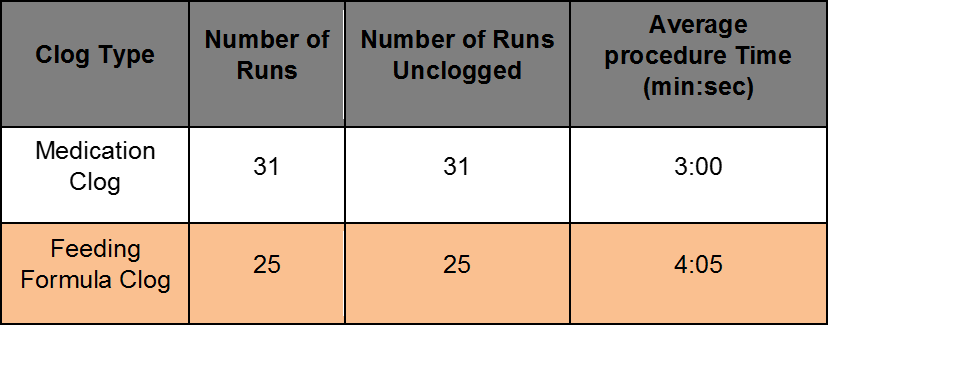
Using the TubeClear System to Clear Clogged G-tubes.
![]()
Benchtop Study evaluated at AMI with Levin 18 Fr, 14 inch long gastrostomy tubes. Half of the occlusions were made from 2:1 ratio of coagulated protein and ground medication (Medication Clog). Half of the occlusions were made from 1:1 ratio of feeding formula and fiber (Feeding Formula Clog).
Using the TubeClear System to Clear Clogged NE tubes.
Benchtop Study evaluated at AMI with Levin 10F Fr, 55 inch long nasoenteral (Entriflex) tubes. Half of the occlusions were made from 2:1 ratio of coagulated protein and ground medication (Medication Clog). Half of the occlusions were made from 1:1 ratio of feeding formula and fiber (Feeding Formula Clog).
References:
1. Ireton-Jones C, DeLegge M. Handbook of Home Nutrition Support. Sudburry, MA: Jones and Bartlett; 2007
2. Beyer PL, Matarese LE, Gottschlich MM. Complications of enteral nutrition. 1998.
3. Pearce C, Duncan H. Enteral feeding. Nasogastric, nasojejunal, percutaneous endoscopic gastrostomy, or jejunostomy: its indications and limitations. Postgrad Med J. 2002;78(918):198-204.
4. Singer AJ, Richman PB, Kowalska A, Thode HC, Jr. Comparison of patient and practitioner assessments of pain from commonly performed emergency department procedures. Ann Emerg Med. 1999;33(6):652-658.
5. Bae KH, Jeong IS. [Pain perception of nurses and pain expression of patients in critical care units]. J Korean Acad Nurs. 2014;44(4):437-445.
6. Penrod J, Morse JM, Wilson S. Comforting strategies used during nasogastric tube insertion. J Clin Nurs. 1999;8(1):31-38.
7. Blumenstein I, Shastri YM, Stein J. Gastroenteric tube feeding: techniques, problems and solutions. World J Gastroenterol. 2014;20(26):8505-8524.
8. TubeClear System- Clears Clogged Feeding Tubes. 2015;http://www.tubeclear.com/