Syringe Force on Clogged Feeding Tubes
Many people think feeding tubes are merely used to deliver nutrition (i.e., feeding formula), however, they deliver life-sustaining medications too – it’s no wonder they tend to clog. At Actuated Medical, Inc., we developed the TubeClear System to keep enteral therapy (medication, nutrition and hydration) being delivered as prescribed.
Article Summary
- Forces required to do air flushes via enteral syringe in feeding tubes with no clog, 1-layer, and 2-layers of feeding formula mixtures were measured.
- Feeding tube clogs, or material build-up on the walls (i.e., 1-layer clogs), may begin forming before becoming noticeably difficult to flush.
- 2-layer clogs required a force that was nearly 5.5 times of the “No Clog” feeding tubes, which was noticeable when flushed by hand.
- The TubeClear System should be used when caregivers notice higher forces during air or water flushes to maintain full patency of feeding tubes.
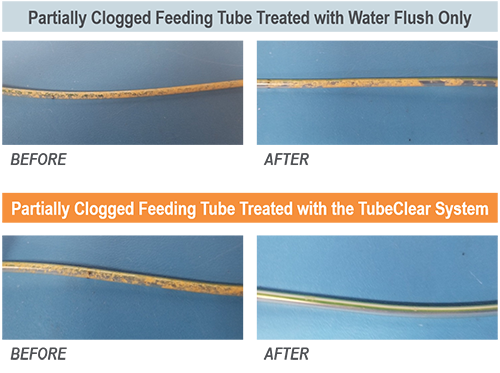
We have demonstrated that compared to flushing with water alone, the TubeClear System can remove residue “sludge” from feeding tube interior walls with greater efficacy.[1] However, the question remains – How does one know when material build-up is adhering to the interior feeding tube wall if fluids can still be introduced into the feeding tube?
For patients using feeding pumps, most pump alarms will sound an alert when the flow rate falls below the predesignated flow rate.[2] However, for those using gravity or syringe feedings, clinicians flush the feeding tube with a syringe to confirm patency (open or unobstructed). These water flushes may require increased force if materials are building up on the inner tube walls. In cases of fully clogged feeding tubes, the water may blow backward toward the clinician due to increased syringe resistance. Note that using excessive force on a syringe (often called power flushing) is generally not recommended as it may cause a rupture to the patient’s feeding tube.[3]
Measuring Flushing Force
Our engineers investigated the amount of force (Newtons [N]) required to be applied to a syringe plunger when attempting to introduce air into non-clogged and partially clogged feeding tubes. In vitro produced clogs were created with a mixture of feeding formula and fiber within 14Fr NG feeding tubes (Cardinal Health, Dublin, OH). Three (3) different feeding tube conditions were tested, N=15 trials, with n=5 trials/feeding tube condition: 1) No clog (lacking all material), 2) 1-layer of clog mixture on feeding tube walls, and 3) 2-layers of clog mixture on feeding tube walls (see Figure 2). To create the single layer, the clog mixture was introduced into feeding tubes (N=10) and dried at 55°C for three (3) hours. To create the two-layer clog buildup, a second clog layer was introduced into a subset of the same feeding tubes (N=5) and dried at 55°C for three (3) hours. To measure the force, a 60-cc syringe was filled with air to the 50-cc mark, and the plunger was depressed to the 10-cc mark using a Shimpo model 100XY force gauge (ELECTROMATIC Equipment Co., Inc., Cedarhurst, NY) (see Figure 1). A n = 5 trials were performed for each feeding tube condition.
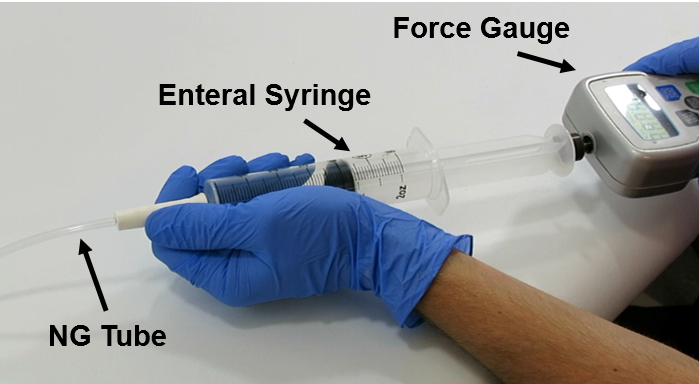
Figure 1: Testing set-up.
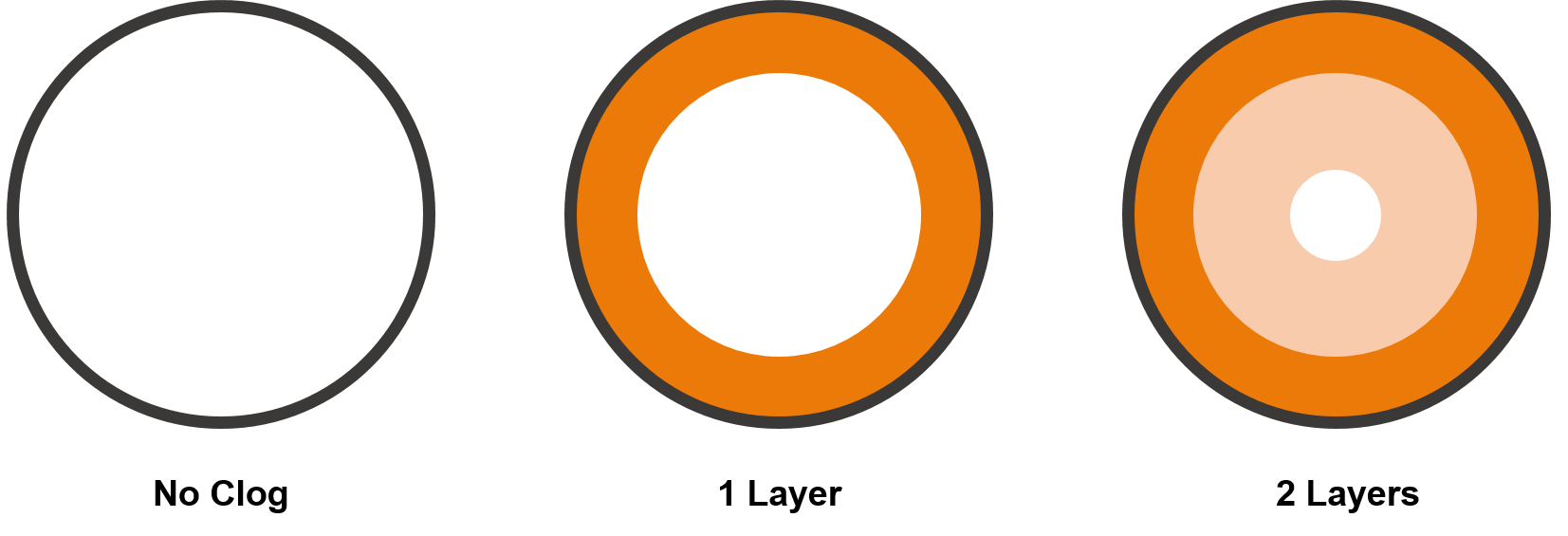
Figure 2: A rendering of the cross-section of the clog types. The grey circle represents the feeding tube wall, and clog material is represented in shades of orange.
The peak force (measured in Newtons [N]) required to push air via the syringe through a non-clogged feeding tube averaged 7.6±0.1N, compared to 14.3±0.5N and 41.0±1.7N, for the one and two layered partially clogged feeding tubes, respectively (see Figure 3).
While these measurements demonstrate an increasing amount of required force, what does that feel like in practice?
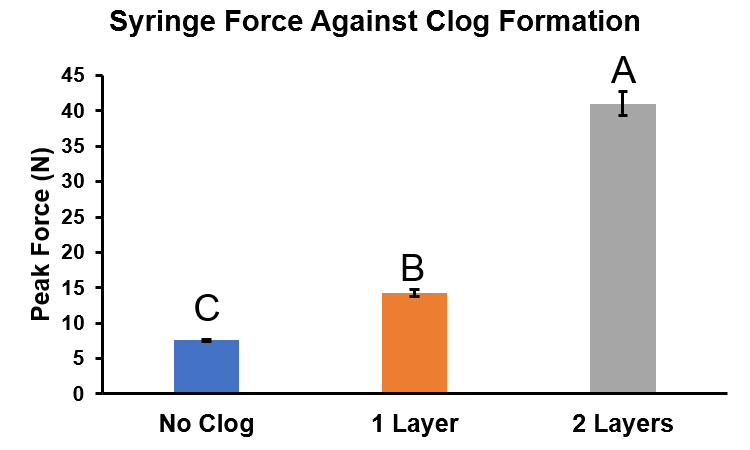
Figure 3: Syringe Force testing summary.
Blue Bar= No clog, Orange Bar= Single layer of clog mixture, Gray Bar= Double layer of clog mixture. n=5 trials/performed for each feeding tube condition. Error bars= standard error of the mean. Two-way ANOVA, Tukey’s Multiple comparison test, different variables =p<0.01.
Feeling the Force
There are many publications discussing preventative means to feeding tube clog formation and multiple ways to remove clogs;[4-5] however, the question as to how one can determine if a feeding tube is fully patent does not appear to have been addressed.
Some feeding tube clogs appear to form quickly, while others occur gradually over time, leading clinicians and care takers to be uncertain to the state of patency of a feeding tube at any particular time. We aimed to quantify the amount of required force to introduce air into feeding tubes with the various levels of clogging- with the end goal to correlate those values with a subjective “feel,” as such, initial tests were conducted without a force gauge. Videos demonstrate how easily (or not) air could be introduced into feeding tubes of the various conditions.
A
B
C
Figure 4: Syringe resistance against each feeding tube condition. A) No clog. B) 1 layer. C) 2 layers (note: looping GIF animation may look like the plunger “snaps” back, but this is the beginning of the animation).
As expected, the feeding tube without a clog (No Clog) could be flushed with air without experiencing any major resistance. However, the feeding tube with a single layer of clog mixture appears to flush almost as easily as the “No Clog” feeding tube, but the required force as measured by the force gauge was nearly double. This finding suggests that feeding tube clogs, or material build-up on the walls, may begin forming before becoming noticeable to clinicians or caretakers. Further research is required to elucidate this finding.
Attempts to flush air into feeding tubes with a double layer of clog mixture proved the most difficult, requiring additional force as the syringe plunger pushed backwards towards the Operator (see Figure 4c) due to the partial blockage. These simulated clogs required a force that was nearly 5.5 times that of the “No Clog” feeding tubes.
From Bench to Bedside
Using the TubeClear System proactively can remove material build-up from feeding tube inner walls enabling enteral therapy (i.e., medication, nutrition and hydration) to be delivered as prescribed.[1] Based on the results presented here, we recommend using the TubeClear System on a patient’s feeding tube as soon as the clinician notices a change in the required pressure to administer fluid or air during routine syringe flushing, as this may be indicative of material build-up on the inner walls of the tube.
References:
- Actuated Medical, Inc. Internal Test Report Doc. No. 1100791569-001.
- Cardinal Health, Dublin, OH. https://www.cardinalhealth.com/content/dam/corp/web/documents/patient-recovery/Literature/kangaroo-connect-enteral-feeding-pump-operator-manual.pdf. Accessed 9/27/19.
- Richards, S., Walsh, K. (2016), Feeding Tube Irrigation: Performing. Nursing Practice and Skill. https://www.ebscohost.com/assets-sample-content/Feeding_Tube_Irrigation_Performing_-_NSP.pdf. Accessed 9/27/19.
- Boullata, J. I., Carrera, A. L., Harvey, L. , Escuro, A. A., Hudson, L. , Mays, A. , McGinnis, C. , Wessel, J. J., Bajpai, S. , Beebe, M. L., Kinn, T. J., Klang, M. G., Lord, L. , Martin, K. , Pompeii‐Wolfe, C. , Sullivan, J. , Wood, A. , Malone, A. , Guenter, P. and , (2017), ASPEN Safe Practices for Enteral Nutrition Therapy. Journal of Parenteral and Enteral Nutrition, 41: 15-103 0148607116673053. doi:1177/0148607116673053.
- Lord, L.M. (2018), Enteral Access Devices: Types, Function, Care, and Challenges. Nutrition in Clinical Practice, 33(1): 16-38. doi: 10.1002/ncp.10019.